
The Common Vein Copyright 2010
Introduction
Fluid attenuated inversion recovery (FLAIR) is used to complement conventional T2 weighted images providing heavily T2 weighted characterization, of the brain parenchyma but nullifying the the signal from the CSF.
Thius any fluid in the brain is intensely white providing excellent contrast between edematous or fluid containing pathology and non edematous tissues.
With the CSF being dark FLAIR provides a contrast for periventricular disease including periventricular infarction and MS plaques. Parial voluming artifct usual for conventional T2 weighted images are thus reduced.
Periventricular Disease |
|
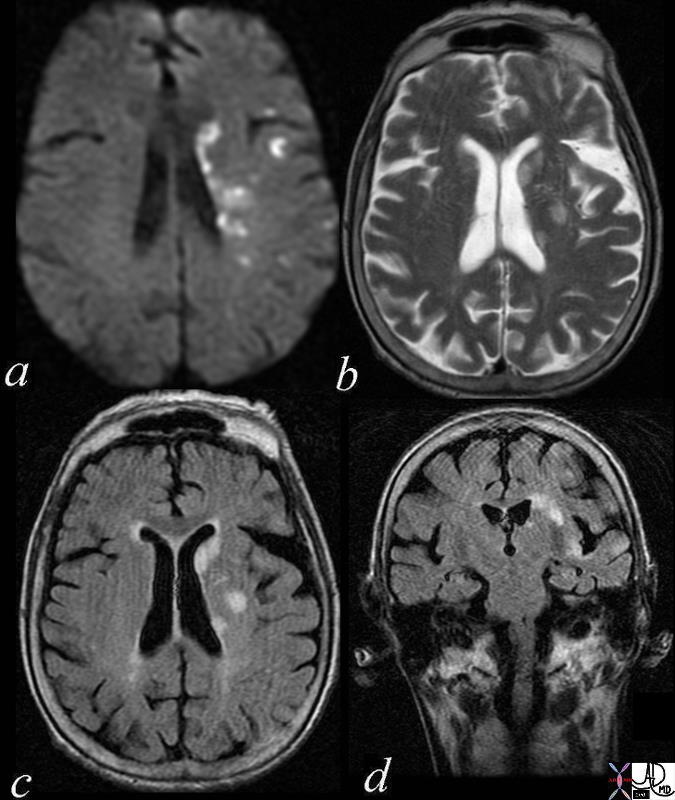
Multicentric Infarcts – Carotid Stenosis The images reveal multicentric acute infarcts in the left cerebral hemisphere involving the internal capsule and left parietal lobe cortex. Image a is the DWI sequence and the high intensity foci are diagnostic of acute infarction. Image b is a T2 weighted image that reflects increase water in the high intensity regions. Image c is an axial FLAIR and d a coronal FLAIR sequence both sensitive to the regions of infarct and characerized by high intensity foci in the regions of acute infarction. Courtesy Ashley Davidoff MD Copyright 2010 72014c01 |
Basal Ganglia and Lenticulostriate Distribution |
|
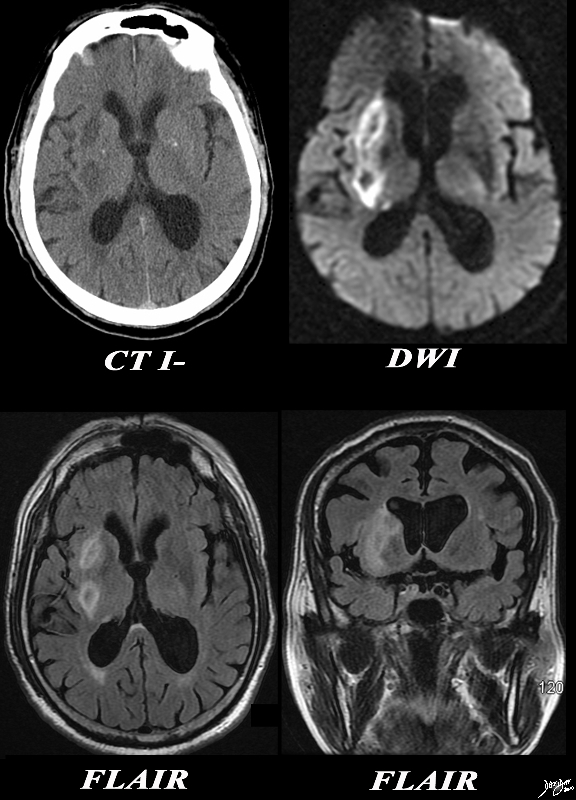
The CT and MRI images are from an 82 year old make with acute neurological deficit. An acute infarction is shown that involves territory within and beyond the basal ganglia. In the CTscan two low density regions are seen medial to the Sylvian fissure and medial to the insular cortex, likely involving the putamen and the part of the right caudate nucleus as well as some white matter in right middle cerebra;l territory. In the second image a high intensity region in the putamen and part of the caudate nucleus is shown together with an area that does not involve the basal ganglia more posteriorly, likely part of the white matter of the right parietal lobe shown in an axial projection on DWI consistent with an acute infarction. The third image is an axial FLAIR sequence and shows the area of parenchymal edema with presumed central necrosis, while the image at low right shows the periventricular disease to better advantage. The constellation of findings is consistent with an acute infarction with distribution of the lenticulostriate vessels arising from the right middle cerebral territory Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89367c01.8s |
Chronic Infarction |
|
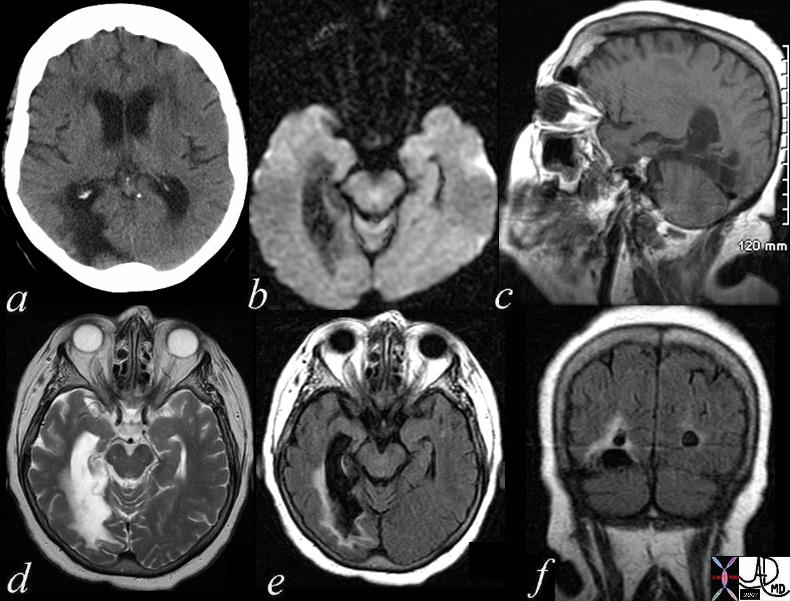
The patient is a 74 year old female with a history of ataxia, incontinence, and memory loss. The MRI shows features of a chronic infarction in the right posterior cerebral artery territory affecting the posteromedial aspect of right temporal lobe and medial and inferior aspect of the right occipital lobe. There is evidence of gliosis with volume loss, atrophy, and encephalomalacia resulting in ex vacuo changes with dilatation of temporal and occipital horns of the lateral ventricles. Image a is a CTscan showing encephalomalacia in the right posterior temporal region and ex vacuo change with ventricular dilatation. Image b is a DWI scan showing no acute changes. Image c is a T1 weighted sagittal view showing no acute hemorrhage. Image d is a T2 weighted study showing compound high intensity changes in the region of the occipital horn but the distinction between disease and dilated ventricle cannot be made because of blooming and isointensity of the ventrciles and the diseases cerebral tissue. Image e is a FLAIR image that turns the CSF black and enables the identification of the high intensity abnormal brain tissue that is smaller than expected after reviewing the T2 weighted image. This case reveals the importance of the FLAIR image. Image f is a coronal FLAIR sequence also showing that the actual dimension of diseased tissue is relatively small. The findings are consistent with an old chronic infarction. Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 71419c01.800 |
Abscess
Demonstrating Edema Around the Abscess |
|
The basal ganglia in the region of the caudate nucleus and globus pallidus are shown in axial projection in this 60 year old female who presents with neurological deficit and a fever. In the first image the focal ill defined mass with mild mass effect is shown in axial projection on a T1 weighted image without contrast (a). The second image with gadolinium shows rim enhancement with mass effect and obstruction of the frontal horn as seen by asymmetric dilatation (b). The third T2 weighted image (c) shows the fluid nature of the cavity and the surrounding edema, mass effect, and accumulation of fluid in the dependant portion of the occipital horn. The fourth image is a FLAIR image and also shows th extent of the edema in the brain The patient had a fever and the constellation of findings were consistent with an abscess of the basal ganglia on the left. In this diagram the relationship of the basal ganglia to the ventricles is demonstrated. Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89054c.8s |
Cysticercosis |
|
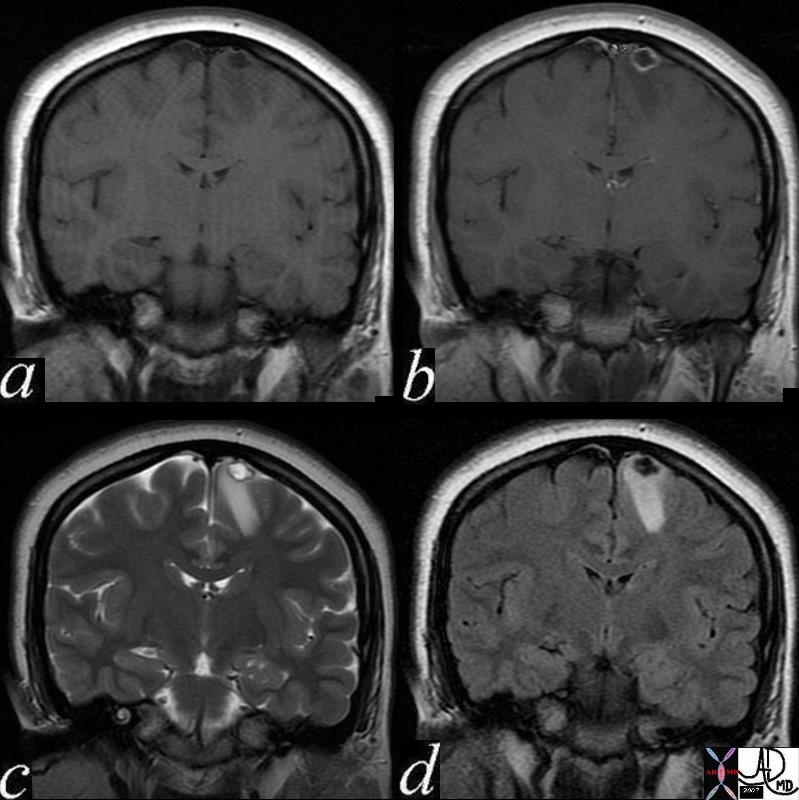
This 24 year old female presented with seizures An MRI with gadolinium enhancement suggested a diagnosis of cysticercosis. Image (a) is a pre gadolinium T1 weighted coronal image showing a hypointense focus in the paramedian part of the frontal lobe. Image (b) shows rim enhancement of the lesion. Image (c) is a coronal T2 weighted image that shows a hyperintense centre with a dark rim. A hypointense scolex can be seen as a tiny linear defect within the cavity. Surrounding edema is present in the white matter. Image(d) is a FLAIR coronal sequence and shows a dark matrix and edema in the surrounding white matter. The linear scolex inside the cavity is seen as relatively hyperintense. These finding are consistent with the diagnosis of cysticercosis. Courtesy Ashley Davidoff MD Copyright 2010 71575c02 |
Neoplasm
|
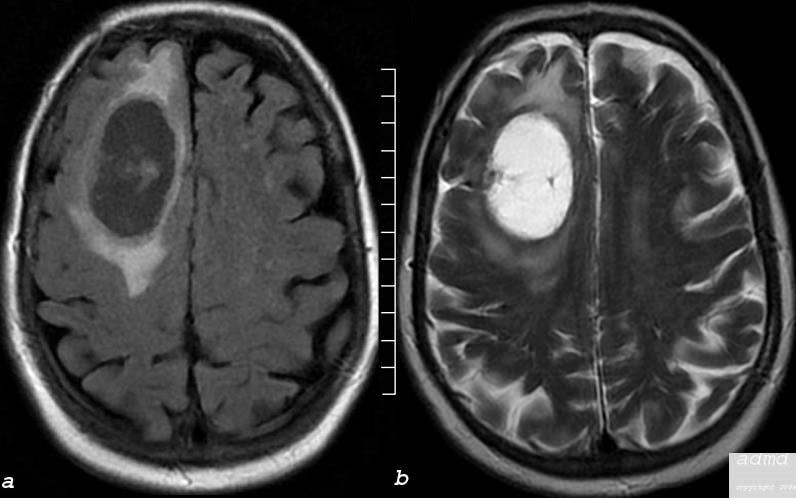
Cystic Metastasis FLAIR (left) and T2 Weighted Images (right) |
|
The MRI performed in the axial plane shows a large mass in the right frontal region and the anterior half of the centrum semiovale. Image (a) is an axial image through the vertex of the brain using FLAIR technique showing mostly a cystic type lesion with some internal thick sepatation with surrounding vasogenic edema. Minimal mass effect on the midline is perceived. Image (b) is an axial T2 weighted sequence showing a cystic matrix and surrounding edema The lesion was shown to be a cavitating squamous cell metastasis brain frontal lobe mass cystic moderate surrounding edema consistent with squamous cell carcinoma metastasis edema involves the anterior half of the right centrum semiovale Courtesy Ashley Davidoff MD Copyright 2010 75408c03 |
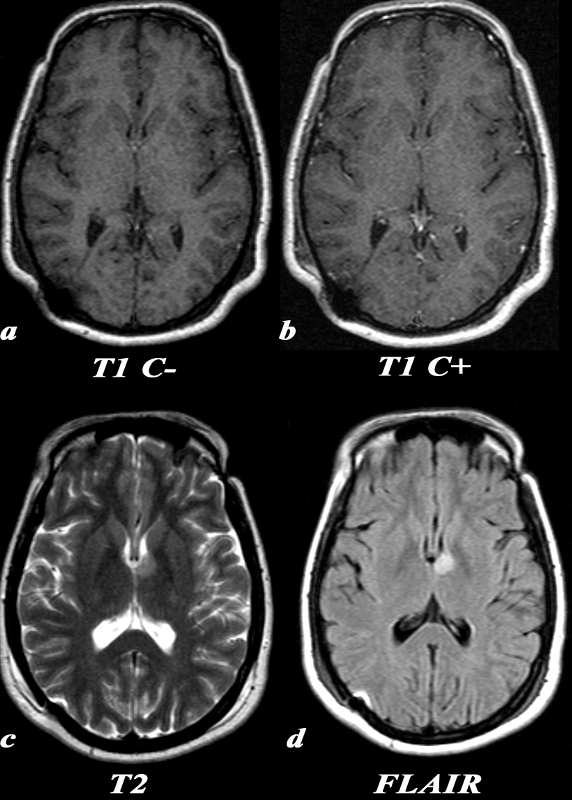
Low Grade Astrocytoma Only Visualized on Water Sensitive Sequences T2 and FLAIR |
|
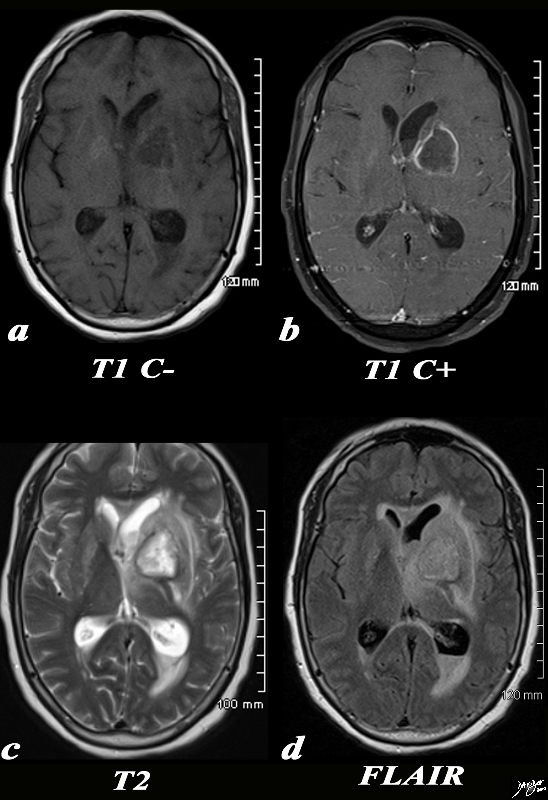
A 31 year old female presented with transient episodes of numbness and tingling in her right face, arm and leg. MRI: T1 C- (a) No definite signal abnormality is identified in the left thalamic low grade glioma. T1 post (T1 C+ b) : Post contrast images demonstrate no enhancement in the region of the known mass. This is typical of a low grade glioma. T2 (c): This T2 weighted image shows a unilateral well circumscribed area of increased signal in the anterior left thalamus. There is no significant mass effect on the adjacent structures. FLAIR (d): This FLAIR image from her MRI demonstrates (with slightly better clarity than the T2 weighted image) a unilateral well circumscribed area of increased signal in the anterior left thalamus. There is no significant mass effect on the adjacent structures. Image Courtesy Elisa Flower MD and Asim Mian MD 97664c.8 |