Subdural Hematoma
The Common Vein Copyright 2010
Definition
When blood collects between the dura and the arachnoid, a subdural hematoma is formed.
It typically results from venous bleeding after blunt head trauma. There is an acceleration-deceleration mechanism, provoking movement of the brain relative to the skull. This ultimately causes rupture of the bridging vessels, thus causing the hemorrhage. In patients in which the brain parenchyma is reduced compared to normal (alcoholics and elderly patients), there is increased risk of vessel rupture through this mechanism.
It is the most common traumatic intracranial hematoma, and, among these, has the highest mortality.
The bleeding may not only be acute, it can also continue and hence be classified as either subacute (3 days to 3 weeks) and chronic (more than 3 weeks). Particularly for slow bleeds causing a chronic presentation, symptoms may be subtle and nonspecific. The hematoma may enlarge significantly before the patient symptoms develop. They include change in mental status with decreased level of consciousness and signs of intracranial hypertension.
Diagnosis is made though imaging. A CT scan of the brain will show a crescent-shaped, concave hematoma. It is usually less dense than an epidural hematoma due to dilution with CSF.
Surgical treatment options include craniotomy and evacuation of the clot.
Fractures – usually tear the dura
Subdural hematoma is the most common dural trumatic injury occurring in the elederly since the brain is shrunken and the vessels are therefore relativley stretched and with trauma they bleed under the dura either immadiately or even subsequently.
The hematoma occurs between the inner layer of the dura and the arachnoid.
A chronic subdural becomes hyperosmolar and th collection slowly draws in fluid and over a few weeks, gets larger and the patient may become unconscious as a result in the subacute phase.
One of the first surgical operations was the relief of subdural hematoma
Structural Considerations
|
Venous Drainage Via the Subarachnoid Space Precarius Position in Trauma |
|
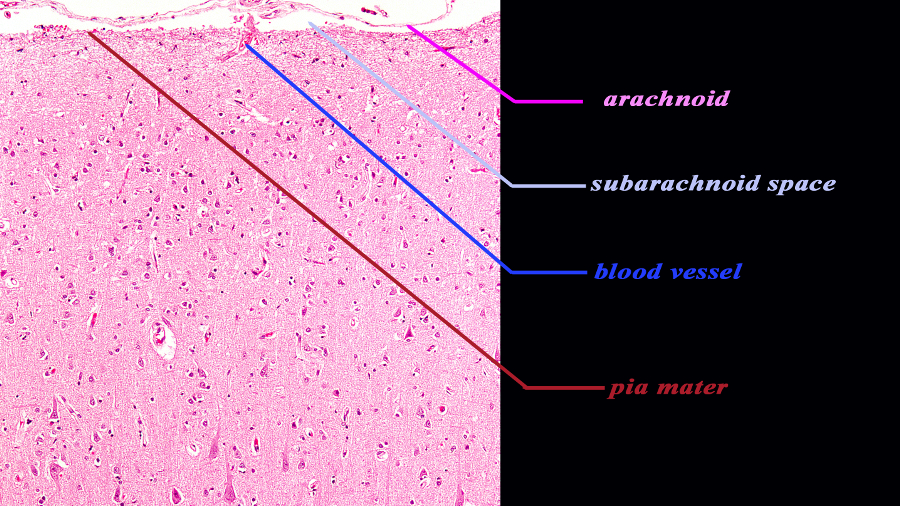
The histological section of the cortex at 10X magnification reveals two of the three meninges of the brain. The inner layer (maroon) is the pia mater and it is in intimate contact with the brain and faithfully follows the sulci and gyri. At this magnification it is barely visible since it is very thin. The second layer is the arachnoid (pink) which is a slightly thicker membrane and follows the pia in a general fashion but does not extend into the sulci. It is intimately attached to the inner layer of the dura The space between the pia and the arachnoid is the subarachnoid space. The blood vessel seen entering the space is likely a small vein. Courtesy of Thomas W.Smith, MD; Department of Pathology, University of Massachusetts Medical School 97377b04.9. |
|
The Subdural Space – A Potential Space Between the Arachnoid and the Dura |
|
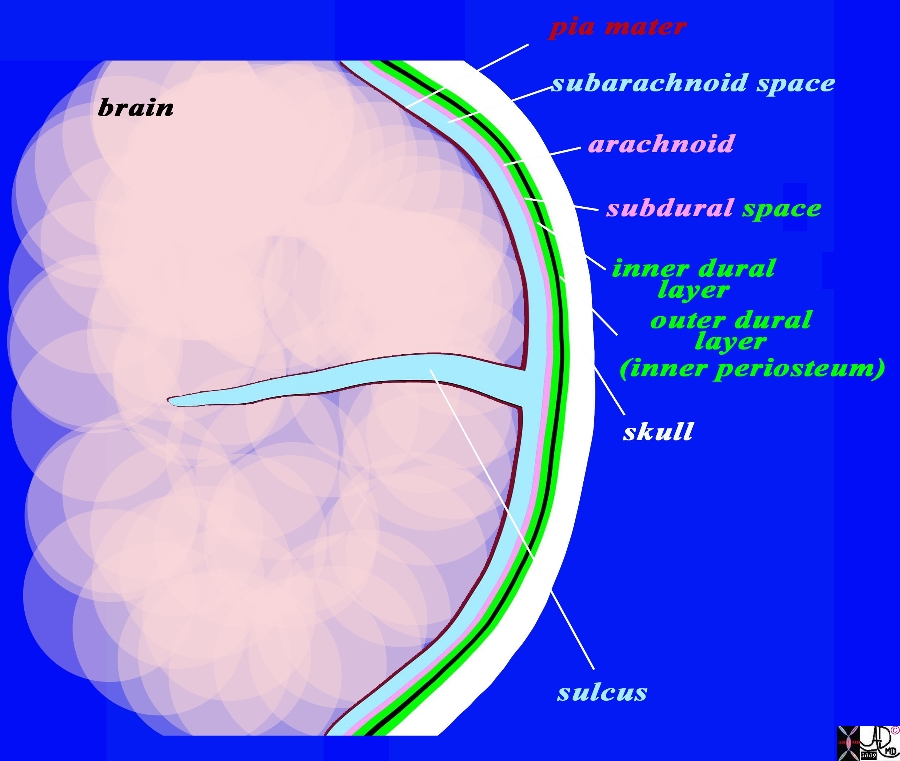
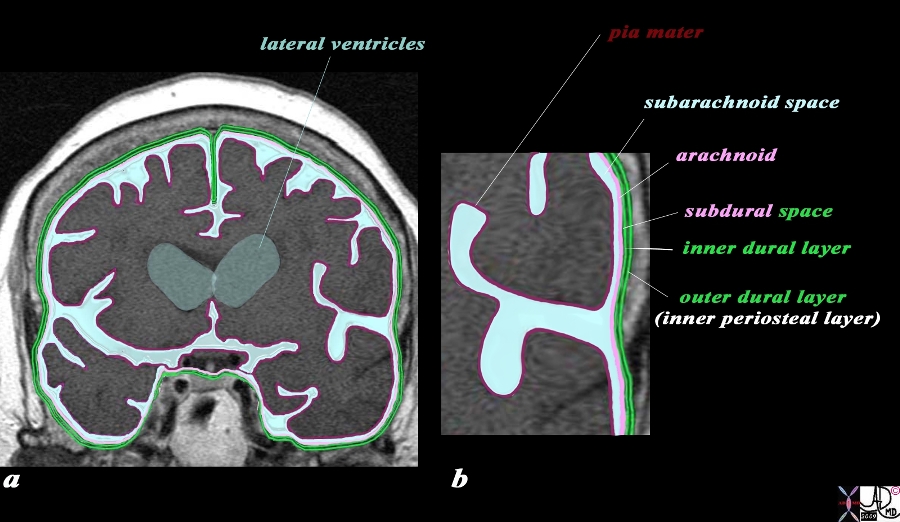
The coronal drawing reveals the three layers of the brain. The inner layer (maroon) is the pia mater and it is in intimate contact with the brain and faithfully follows the sulci and gyri. The second layer is the arachnoid (pink) which is a slightly thicker membrane and follows the pia in a general fashion but does not extend into the sulci. It is intimately attached to the inner layer of the dura (bright green) The space between the pia and the arachnoid is the subarachnoid space, and it is in this space that the CSF is present and surrounds the brain. The next layer is the dura which is a double layer. The inner layer (bright green) is intimately attached to the arachnoid and the outer layer (also bright green) is attached to the bone and functions as the inner periosteum. There is a potential space between the arachnoid (pink) and the inner layer of the dura (green). This space is called the subdural space. (combination pink and green) The CSF (light blue) is seen in the subarachnoid space and in the lateral ventricles (gray blue) c Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 71422.800b02g06.91s |
|
Dura and Arachnoid and Subarachnoid Space MRI T1 Weighted Coronal View |
|
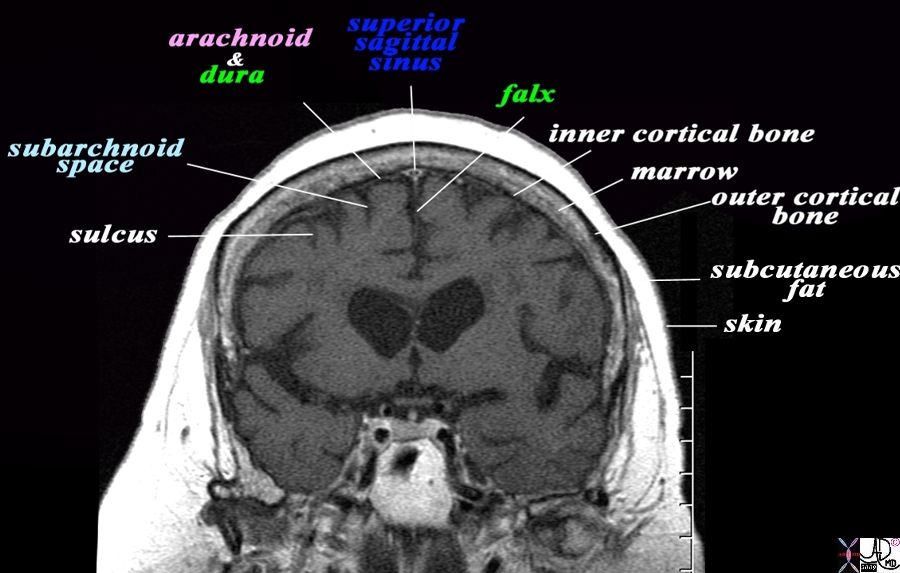
The coronal T1 weighted MRI reveals demonstrates some of the anatomical features of the meninges and their relations The sulci are seen as T1 dark CSF containing fissures in the brain substance. The pia is too thin to see but would be adherent to the brain surface. The space that contains the CSF is called the subarachnoid space (light blue). The very fine T2 bright membrane seen on the surface of the brain is a combination of arachnoid (pink) adherent to the two layers of the dura (green). The outer layer of the dura acts as the inner periosteum and is adherent to the skull. The dura splits at the vertex to encompass the superior sagittal sinus and then extends down in the interhemispheric fissure to form the falx. The thin black T1 dark layer after the arachnoid and dura is the inner cortical bone, and is followed by the T1 bright fat containing marrow of the skull. Next is the thin black T1 dark outer cortical bone, followed by a thick layer of T1 bright subcutaneous fat, and then a thin layer of isointense (to soft tissue) skin layer. Image Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 71422.800bL01.9 |
Dura and Arachnoid and Subarachnoid Space MRI T1 Weighted Coronal View |
|
The coronal image of the brain using T1 weighted MRI sequence reveals the three layers of the brain. The inner layer (maroon) is the pia mater and it is in intimate contact with the brain and faithfully follows the sulci and gyri. The second layer is the arachnoid (pink) which is a slightly thicker membrane and follows the pia in a general fashion but does not extend into the sulci. It is intimately attached to the inner layer of the dura (bright green) The space between the pia and the arachnoid is the subarachnoid space, and it is in this space that the CSF that surrounds the brain is housed. The next layer is the dura which is a double layer. The inner layer (bright green) is intimately attached to the arachnoid and the outer layer (also bright green) is attached to the bone and functions as the inner periosteum. There is a potential space between the two layers of the dura. The CSF (light blue) is seen in the subarachnoid space and in the lateral ventricles (gray blue) Image Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 71422.800b04c01.9s |
The dura mater also has three major reflections. The falx (sickle) cerberi, is a sickle shaped reflection of dura that projects between the cerebral hemishpheres in the interhemispheric fissure vertically, and incompletely divides the two cerebral hemispheres. It has attachments to the ethmoid bone (crista galli) anteriorly. Posteriorly, it attaches to another dural fold, the tentorium (tent) cerebelli.
The tentorium is a horizontal dural reflection which divides the cerebellum and divides the brain into a supratentorial compartment and an infratentorial compartment. The tentorium attaches to the occipital bone of the skull posteriorly. The anterior part of the tentorium is open allowing the brainstem to passes. This opening is called the tentorial notch.
Acute Subdural Hematoma

Bilateral Subdural Hematomas |
| In this patient the non contrast CTscan reveals small bilateral subdural hematomas .
In the left frontal region there is a subgaleal hematoma and underlying the hematoma there is a small hyperdense subdural hematoma in the region of the Sylvian fissure. A contracoup injury manifesting also as a subdural hematoma is seen in the right posterior parietal region. There are linear hyperdensities overlying the frontal lobes bilaterally that may represent small acute hemorrhages as well. Courtesy Ashley Davidoff MD Copyright 2010 70000.800 |
|
Acute Falcine and Frontal Subdural Hemorhage |
|
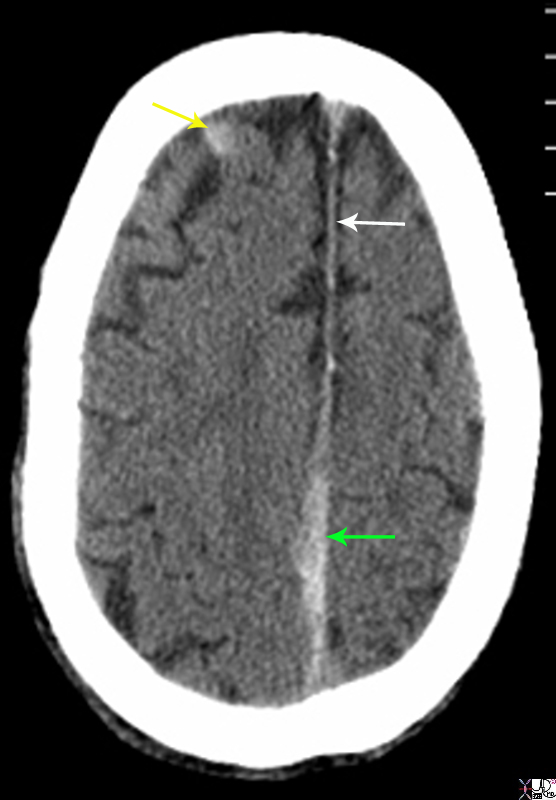
The non enhanced CTscan is from a 80 year old male on coumadin who sustained trauma to the head. There are two acute subdural hemorrhages. The first is a falcine subdural (green arrow) that has resulted in thickening irregularity and increased density of the falx near the vertex. This is contrasted to the normal falx anteriorly (white arrow) The second acute subdural is in the right frontal region (yellow arrow). Courtesy Ashley Davidoff MD Copyright 2010 89283.8sL |
Subacute Subdural Hematoma
Subacute Subdural Hematoma |
|
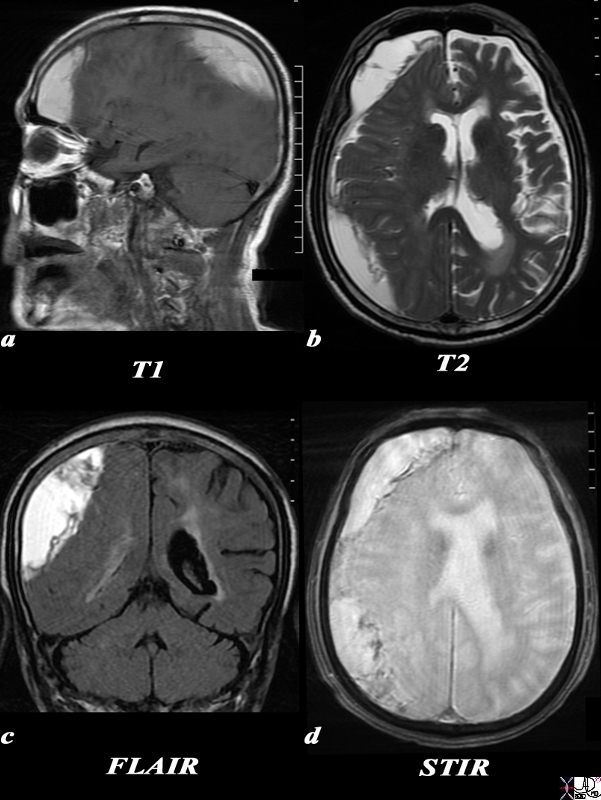
The MRI scan is of a 75year old male and was performed following trauma and change in level of consciousness. The MRI confirms the presence of a large collection overlying the right temperoparietal region . The collection is large and crosses the region of the skull sutures placing it in the subdural space The T1 weighted image (a) shows a hyperintense collection suggesting the presence of methemoglobin. The T2 sequence (b) and FLAIR sequence is also hyperintense suggesting the presence of extracellular methemoglobin. The STIR sequence (c) and to lesser extent the T2 sequence show early rim blackening suggesting the presence of hemosiderin. The effacement of the right lateral ventricle seen on the axila T2 weighted image (b), the coronal FLAIR image (c) and the STIR image (d) suggest mass effect These findings suggest a diagnosis of a large subacute subdural hematoma. With mild mass effect and mild midline shift Courtesy Ashley Davidoff MD Copyright 2010 90443c.8S |
Acute on Chronic Subdural Hematoma
Acute on Chronic Left Fronto-parietal Subdural Hematoma |
|
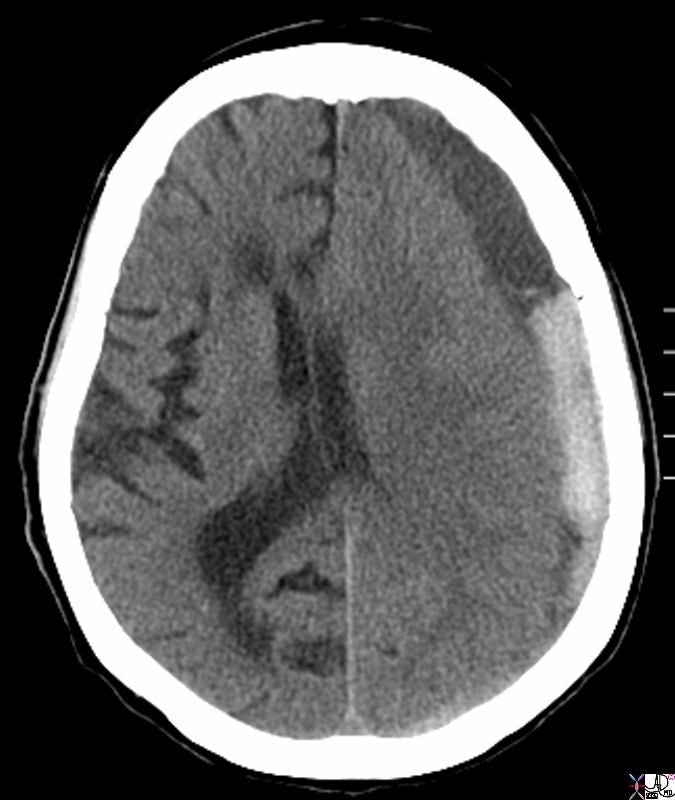
The CTscan without contrast is from a 88 year old male who has a history of falling and recently sustained head trauma and complaining of a severe headache. The scan shows a collection in the left fronto-parietal collection with both high density and low density components. The left frontoparietal collection is subdural hematoma since it crosses suture lines, with the outer border conforming to the shape of the skull . Associated findings include flattening of the right sided frontal sulci and parietal sulci as well as shift of the midline structures typified by the displacement of the septum pellucidum and effacement of the left lateral ventricle. The combination of low density and high density fluid in the subdural collection is consistent with an acute on chronic accumulation Courtesy Ashley Davidoff MD Copyright 2010 97723.8s |
Complex Chronic Subdural Hematoma
|
Subacute Subdural hematoma with Enhancing and Thickened Arachnoid CT scan |
|
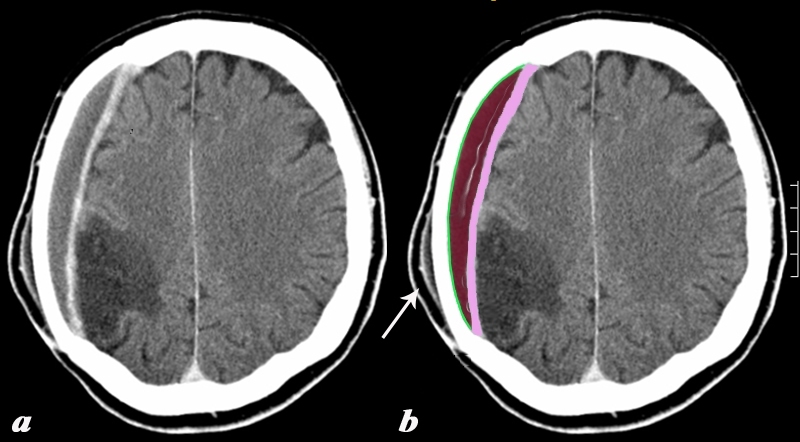
The CTscan with contrast shows a collection that conforms to the shape of the skull with an enhancing meningeal layer. The right parietal collection is a subdural hematoma (SDH) with the outer border conforming to the shape of the skull and lined by the two layers of dura (green) and the inner border thickened and enhancing lined by the arachnoid (pink). The arachnoid is unusually thick in this case suggesting some complexity to the subdural. In the appropriate clinical setting this could be an infected subdural. A subacute subgaleal subcutaneous hematoma is seen in the soft tissues overlying the SDH (white arrow). It also has a slightly enhancing outer layer In addition, as an unrelated abnormality, there is a chronic infarct of the right parietal lobe characterized by a hypodense triangular defect, with loss of gray white matter interface, all consistent with encephalomalacia. Courtesy Ashley Davidoff MD Copyright 2010 89273c03 |
Isodense SDH

Bifrontal Isodense Subdural hematomas CT scan |
|
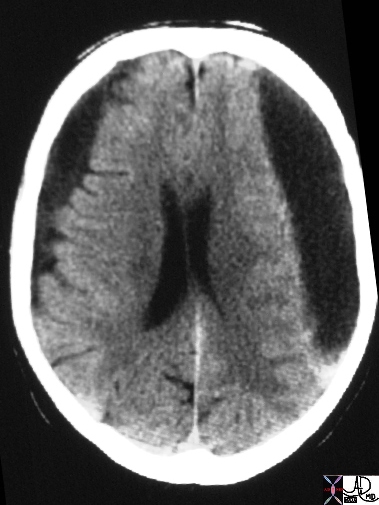
The CTscan without contrast is from a 36 year old male who has a history of a severe headache. The scan shows bilateral bifrontal isodense collections There are no significant associated findindings These findings are consistent with bilateral subacute or chronic isodense subdurals. Courtesy Ashley Davidoff MD Copyright 2010 17354.8 |
Low Density Bilateral Hygromas
|
Chronic Bilateral Subdurals – Hygromas |
|
The CT scan shows bilateral low density extraaxial collections that compress the brain substance with no evidence of midline shift. In the chronic phase of SDH’s the red cells and fibrinous elements of the hematoma resorb and low density fluid cotaining hematomas remain. These are called hygromas since they are filled with fluid. Image Courtesy Courtesy Ashley Davidoff MD 15634 |