
Copyright 2010
Introduction
Medulloblastoma – Most Common Malignant Brain Tumor of Childhood |
|
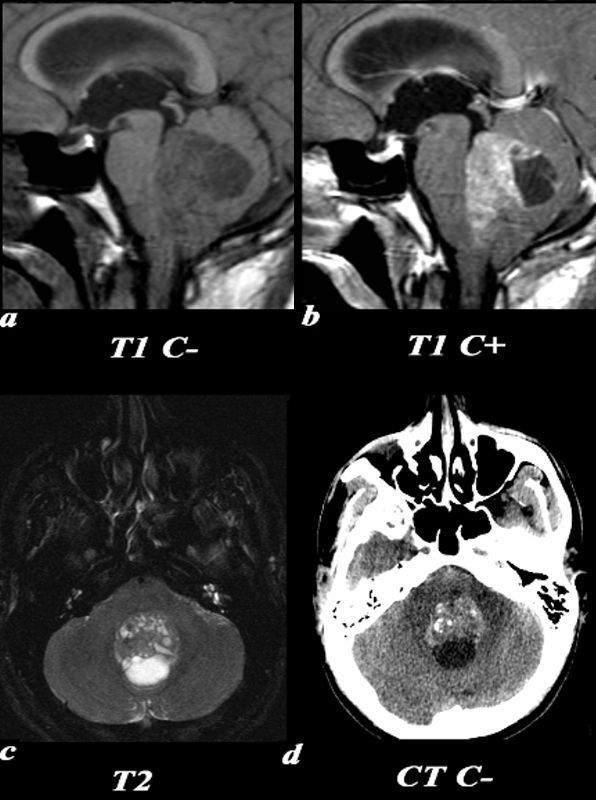
This 26 year old male presented with a three week history of progressive headache, nausea and vomiting. T1 pre (a) and post (b,): The exact origin of this mass can be difficult to ascertain given its large size. It clearly grows into the fourth ventricle, widening the lower portion of the Sylvian aqueduct. Note the smooth interface with the posterior aspect of the pons with associated mass effect verses the more irregular margin posteriorly where it arises from the cerebellum. T2 (c): The solid component of the medulloblastoma matches gray matter signal. Cystic or necrotic areas are demonstrated by higher T2 signal areas. CT(d): The unenhanced CT scan demonstrates a predominately hyperdense mass with punctuate calcifications in the region of the fourth ventricle . The low density area posteriorly is a cystic or necrotic component of the mass while the fourth ventricle is completely effaced. Image Courtesy Elisa Flower MD and Asim Mian MD 97668c01.81 |
Hemangioblastoma in the Cerebellum Mural Nodule within a Cystic Lesion |
|
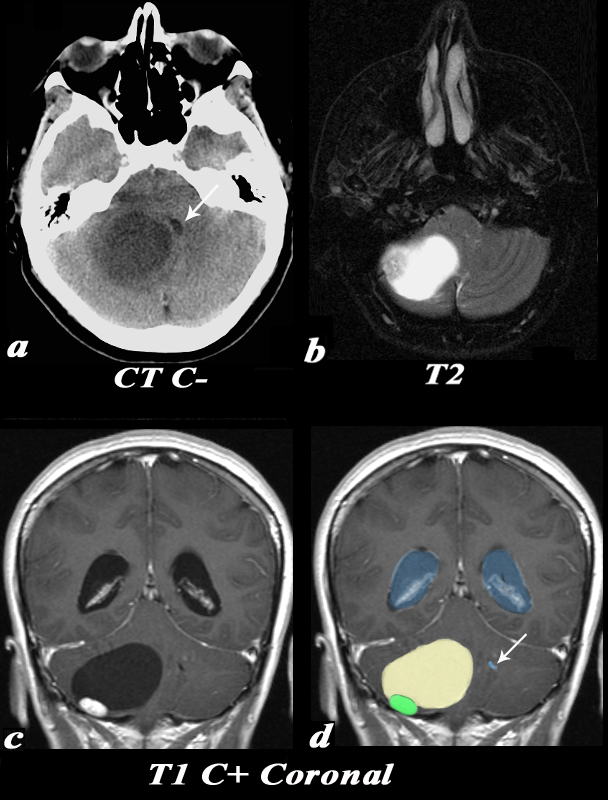
This 55 year old female complained of an occipital headache for one month with increased difficulty ambulating. CT: Noncontrast CT image (a) demonstrates a large low density lesion in the right cerebellum. This lesion causes significant mass effect on the fourth ventricle which is displaced towards the left (white arrow). This mass effect caused obstruction of the CSF pathway resulting in obstructive hydrocephalus and subsequent symptoms. MRI: The T2 weighted image (b) demonstrates a predominantly T2 hyperintense cystic lesion with a nodular T2 isointense component seen laterally. Post contrast T1 weighted coronal images (identified by high signal in the venous sinuses demonstrate the classic cyst (light yellow in d) with mural nodule (green in d) appearance of a hemangioblastoma. Note the enlarged lateral ventricles (blue) and the displaced and compressed 4th ventricle (white arrow d). Image Courtesy Elisa Flower MD and Asim Mian MD 97652c01.81 |
Craniopharyngioma |
|
This six year old male has a heterogeneous mass in the suprasellar region. CT: (a,b) These are images from two slightly different levels which demonstrate the heterogeneous nature of a craniopharyngioma. There is a superior predominantly cystic area with thin peripheral calcification (a). The more solid component inferiorly to the left demonstrates more solid calcification and can be identified in both soft tissue and bony window/level settings. These findings are consistent with a craniopharyngioma. Image Courtesy Jimmy Wang MD 97636c.8 |
Central neurocytoma Small Cysts appreciated only on the T2 weighted image (c) |
|
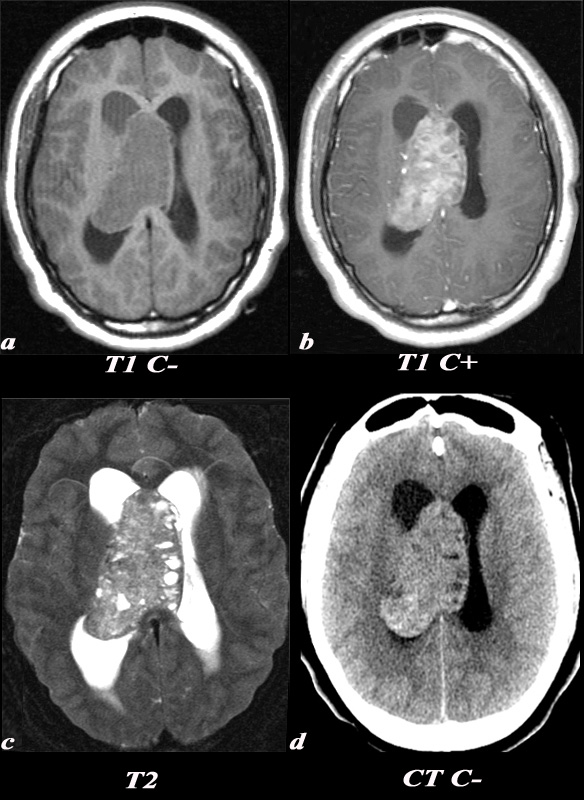
A 21 year old female was found to have papilledema on physical exam noted by her optometrist. MRI: T1 pre (T1 C- a) and post (T1 C+ b): Post contrast images demonstrate the heterogeneous enhancing nature of this mass. These images demonstrate centered in the right lateral ventricle with involvement of the septum pellucidum and partial extension into the left lateral ventricle. T2: T2 weighted images demonstrate internal areas of high signal consistent with cystic components. Also note the high T2 signal adjacent to the enlarged lateral ventricles which is a finding consistent with hydrocephalus, classically called transependymal flow of CSF. This unenhanced CT scan also demonstrates the mass in the right lateral ventricle with similar features of heterogeneity and involvement of the septum pellucidum and partial extension into the left lateral ventricle. Notice the internal low density or cystic components and the higher density calcifications seen posteriorly. The lateral ventricles are enlarged consistent with resultant hydrocephalus. These findings are consistent with a diagnosis of central neurocytoma. Image Courtesy Elisa Flower MD and Asim Mian MD 97634c01.8s |
Desmoplastic Infantile Ganglioglioma |
|
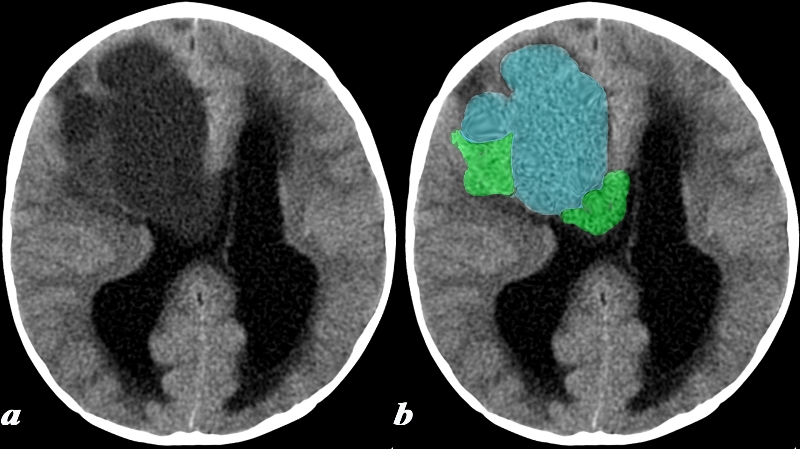
This 17 month old boy presented with vomiting. CT: (a,b) A noncontrast head CT was obtained and demonstrates a predominantly cystic lesion (blue) with more solid components (green) at the periphery. Notice the enlargement of the lateral ventricles which is due to obstructive hydrocephalus caused by obstruction at the level of the third ventricle (not included on this image). These findings are consistent with a desmoplastic infantile ganglioglioma (DIG) Image Courtesy Elisa Flower MD and Asim Mian MD 97641c.8 |

Hyperdense Colloid Cyst |
|
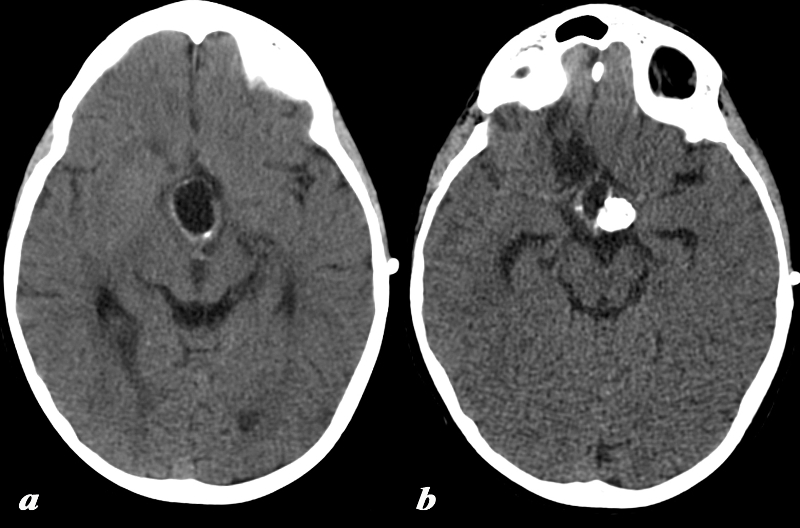
The CT scan is from a young adult female who presented with a history of trauma and a subcentrimetre hyperdense lesion identified was an incidental finding. On the non contrast CT a smooth round hyperdense nodule is noted in the region of the foramen of Munro and the anterior aspect of the third ventricle. These findings are consistent with a diagnosis of a colloid cyst. Pathologically these lesions are benign Courtesy Ashley Davidoff MD copyright 2010 All Rights Reserved 70045.800 |