
Calcium in the Brain
The Common Vein Copyright 2010
Introduction
|
Age Related Benign Calcification |
|
Calcification in the basal ganglia in the region of the globus pallidus is shown in axial projection in this CTscan. Aside from mild brain atrophy the scan is normal Age related dystrophic calcification of the basal ganglia is usually a benign finding in the elderly Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 77120.8 |

Unilateral Benign Calcification |
|
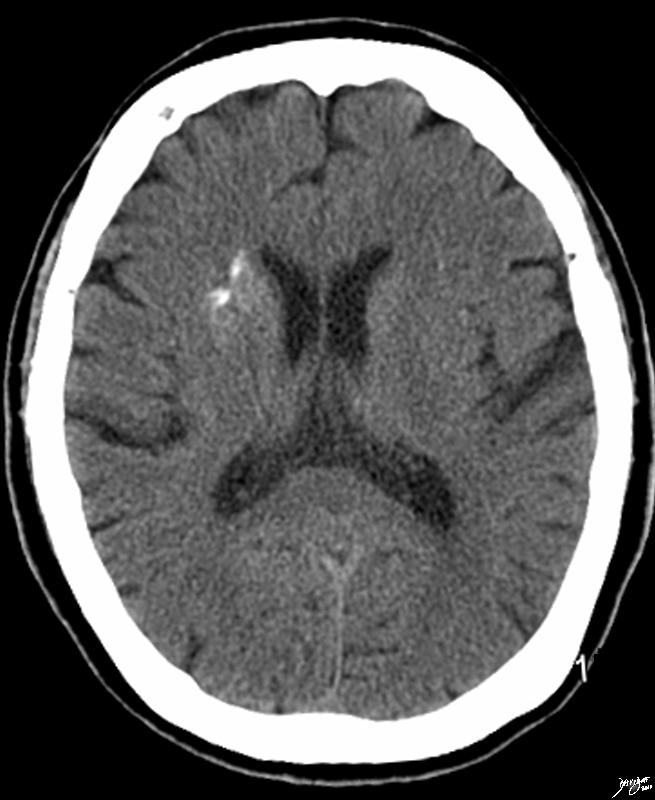
Unilateral calcification in the basal ganglia in the region of the caudate nucleus, globus pallidus and putamen is shown in axial projection in this CTscan of a 69 year old male. The scan is otherwise normal Age related dystrophic calcification of the basal ganglia is usually a benign finding. Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89074.8 |
|
Basal Ganglia Calcification in Sarcoidosis |
|
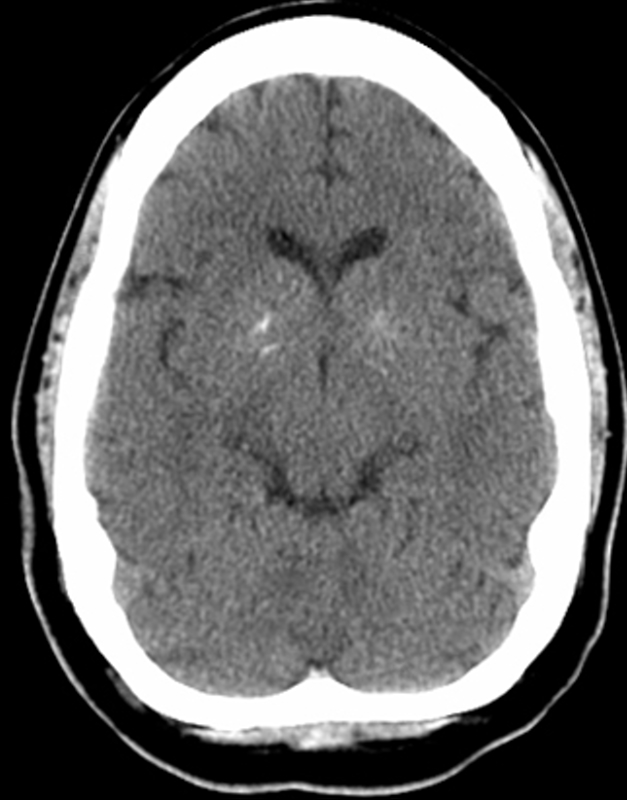
Calcification in the basal ganglia in the region of the globus pallidus is shown in axial projection in this CTscan of a 29 year old female with sarcoidosis. The scan is otherwise normal. It is likely that there is granulomatous involvement of the basal ganglia with sarcoidosis Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89070.8 |
|
Basal Ganglial Calcification in Psychiatric Disease |
|
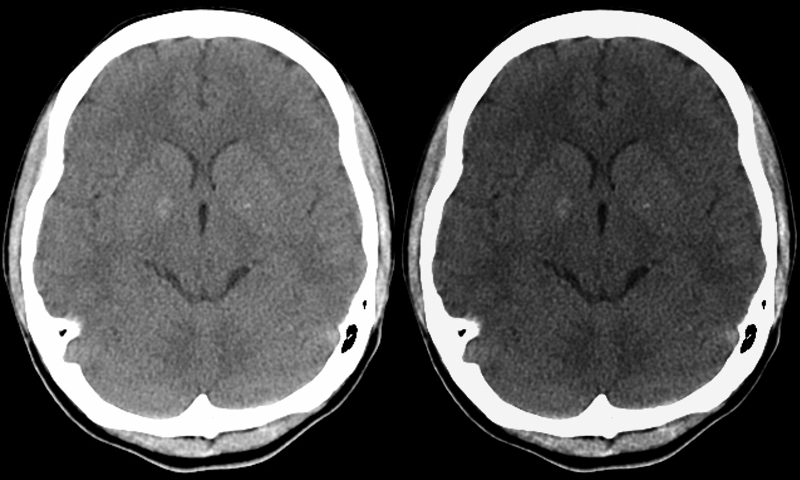
Calcification in the basal ganglia in the region of the globus pallidus is shown in axial projection in this CTscan of a 26 year old female with history of psychiatric disease. The scan is otherwise normal. The windows have been narrowed in the image on the right to accentuate the calcification The association of premature calcification of the basal ganglia with psychiatric illness is well established Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89070c.8 |
|
Basal Ganglia Calcification |
|
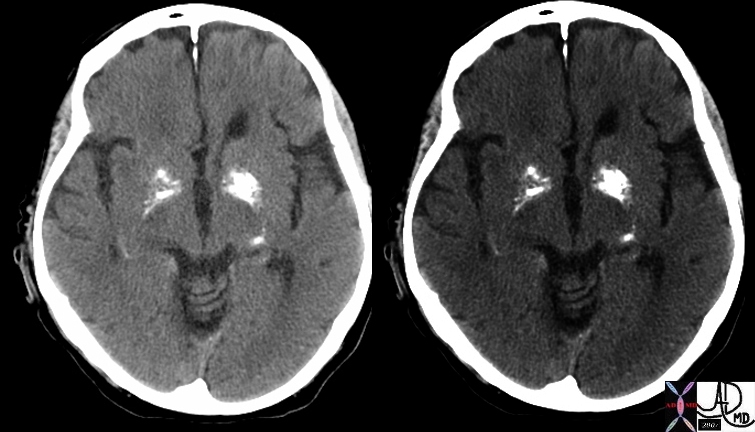
In this patient there is more than the usual calcification in the basal ganglia, and more specifically the globus pallidus. Calcification is usually considered as dystrophic or metastatic. Most benign cases are age related and are due to dystrophic calcification. When calcification is heavy then metastatic calcification should be considered and diseases such as hyperparathyroidism should be considered. Heavy calcification is also seen with Fabry’s disease which is a rare genetic abnormality resulting in deposition of glycolipids in tissues Courtesy Ashley Davidoff MD 48702c01 |
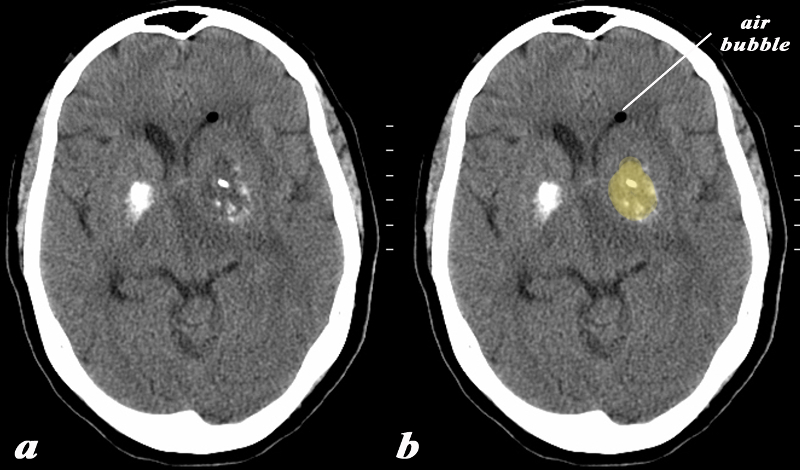
Calcium and a Mass in ther Basal Ganglia Air in the Ipsilateral ventricle An Evolving Abscess |
|
The basal ganglia in the region of the caudate nucleus and globus pallidus are shown in axial projection in this 60 year old female who presents with neurological deficit and a fever. The CT scan shows asymmetric calcification in the region of the caudate nucleus and globus pallidus. The calcifications on the left are expanded by a low density presumably fluid collection (yellow). There is associated surrounding edema and mass effect on the ipsilateral ventricle. A small air bubble is noted in the anterior most portion of the left frontal horn. There is mild midline shift An MRI confirmed the presence of a complex fluid in the left basal ganglion and significant surrounding edema. The patient had a fever and the constellation of findings were consistent with an abscess of the basal ganglia on the left. In this diagram the intimate relationship of the basal ganglia to the ventricles is exemplified by the ipsilateral mass effect and the presence of air presumably from gas forming organisms. Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89065c01.8 |
Neoplasm
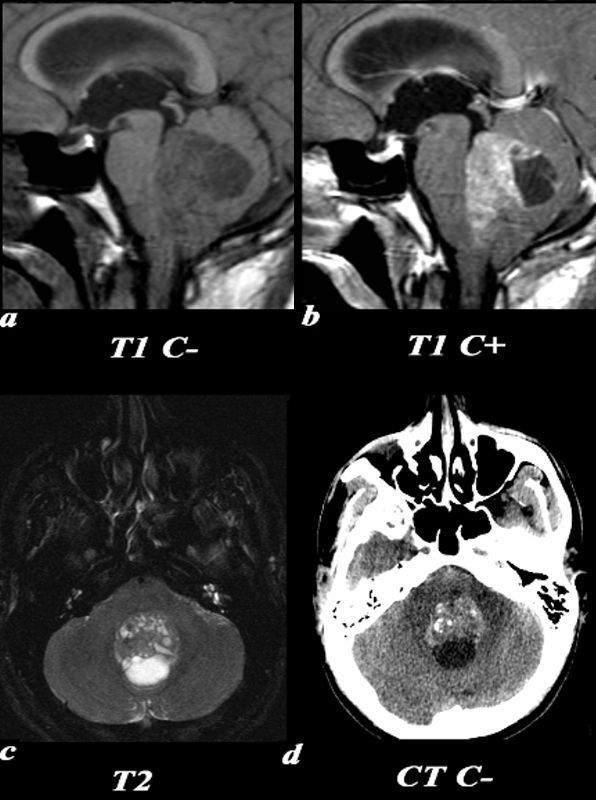
Medulloblastoma – Most Common pediatric MAlignant Brain Tumor CTscan is Sensitive to Calcification |
|
This 26 year old male presented with a three week history of progressive headache, nausea and vomiting. T1 pre (a) and post (b,): The exact origin of this mass can be difficult to ascertain given its large size. It clearly grows into the fourth ventricle, widening the lower portion of the Sylvian aqueduct. Note the smooth interface with the posterior aspect of the pons with associated mass effect verses the more irregular margin posteriorly where it arises from the cerebellum. T2 (c): The solid component of the medulloblastoma matches gray matter signal. Cystic or necrotic areas are demonstrated by higher T2 signal areas. CT(d): The unenhanced CT scan demonstrates a predominately hyperdense mass with punctuate calcifications in the region of the fourth ventricle . The low density area posteriorly is a cystic or necrotic component of the mass while the fourth ventricle is completely effaced. Image Courtesy Elisa Flower MD and Asim Mian MD 97668c01.81 |
Craniopharyngioma Rim Calcification and Chunky Calcififcation |
|
This six year old male has a heterogeneous mass in the suprasellar region. CT: (a,b) These are images from two slightly different levels which demonstrate the heterogeneous nature of a craniopharyngioma. There is a superior predominantly cystic area with thin peripheral calcification (a). The more solid component inferiorly to the left demonstrates more solid calcification and can be identified in both soft tissue and bony window/level settings. These findings are consistent with a craniopharyngioma. Image Courtesy Jimmy Wang MD 97636c.8 |
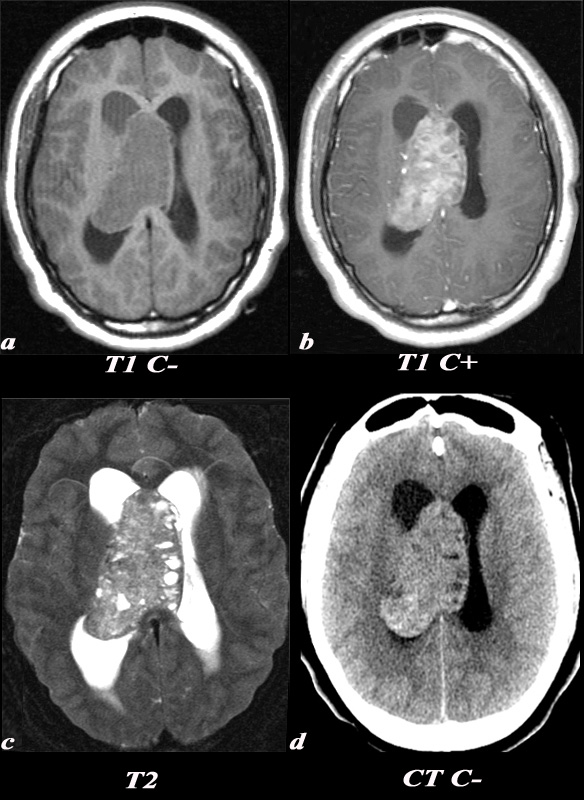
Central Neurocytoma Fine calcification seen only in the posterior aspect of the mass on CT |
|
A 21 year old female was found to have papilledema on physical exam noted by her optometrist. MRI: T1 pre (T1 C- a) and post (T1 C+ b): Post contrast images demonstrate the heterogeneous enhancing nature of this mass. These images demonstrate centered in the right lateral ventricle with involvement of the septum pellucidum and partial extension into the left lateral ventricle. T2: T2 weighted images demonstrate internal areas of high signal consistent with cystic components. Also note the high T2 signal adjacent to the enlarged lateral ventricles which is a finding consistent with hydrocephalus, classically called transependymal flow of CSF. This unenhanced CT scan demonstrates also demonstrates the mass in the right lateral ventricle with similar features of heterogeneity and involvement of the septum pellucidum and partial extension into the left lateral ventricle. Notice the internal low density or cystic components and the higher density calcifications seen posteriorly. The lateral ventricles are enlarged consistent with resultant hydrocephalus. These findings are consistent with a diagnosis of central neurocytoma. Image Courtesy Elisa Flower MD and Asim Mian MD 97634c01.8s |
Oligodendroglioma Paramagnetic Effect of the Calcium |
|
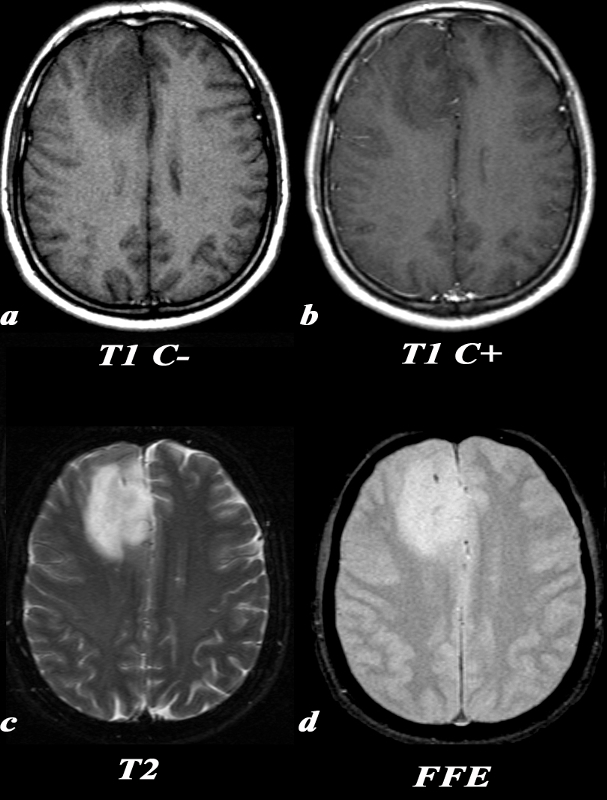
This 35 year old male presented with new onset of seizure. T1 C- (a): On this T1 weighted image, there is a hypointense region in the right frontal lobe with blurring of the normally clear gray-white matter distinction. T1 post C+ (b): No definite areas of enhancement were identified in this mass which is occasionally the case in oligodendrogliomas. T2 (c): On T2 images, this lesion is more clearly defined as a region of increased signal. There is expansion of the involved gyri, as the adjacent sulci are not as clearly seen as they are in the same region on the contralateral side. Note the relative lack of surrounding edema around the lesion which would have the appearance of increased signal in the adjacent white matter sparing the gray matter. FFE(d): This gradient echo MRI sequence is tailored for picking up substances which alter the local magnetic field, or paramagnetic substances, which will appear hypointense. This “blooming” can be seen in areas of calcification, as in this case. Calcification is seen in a majority of oligodendrogliomas. Image Courtesy Lawrence Chin MD 97673c.8 |

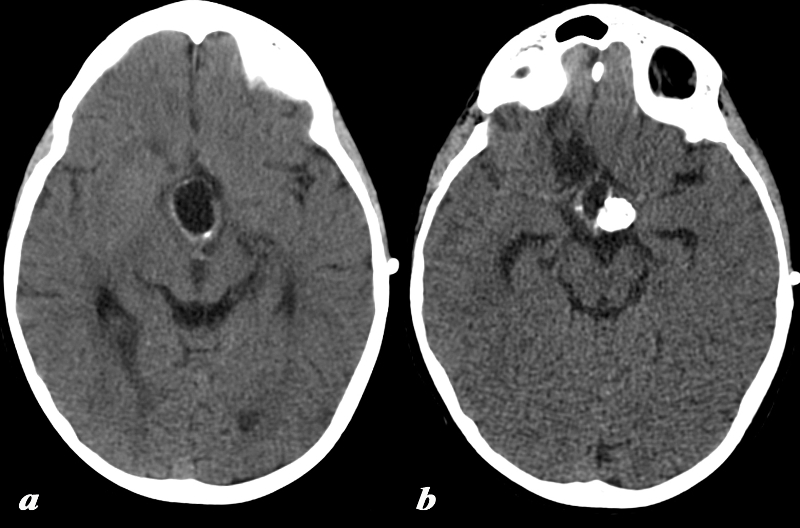
Colloid Cyst of the Third Venticle – Calcified Cholesterol Crystals |
|
The CT scan is from a young adult female who presented with a history of trauma and a subcentrimetre hyperdense lesion identified was an incidental finding. On the non contrast CT a smooth round hyperdense nodule is noted in the region of the foramen of Munro and the anterior aspect of the third ventricle. These findings are consistent with a diagnosis of a colloid cyst. Pathologically these lesions are benign and filled with gelatinous material and cholesterol crystals which are responsible for the hyperdensity. They can rupture or cause hydrocephalus. b Courtesy Ashley Davidoff MD copyright 2010 All Rights Reserved 70045.800 |
References
Erini Makariou, MD, and Athos D. Patsalides, MD, Intracranial calcifications Applied Radiology on Line Volume 38, Number 11, November 2009