
Craniopharyngioma
The Common Vein Copyright 2010
Definition
A craniopharyngioma is a histologically benign neoplasm which is generally located in the sellar and suprasellar region. They can, however, be quite large and locally aggressive. They are thought to arise from remnants of the Rathke’s pouch. There is a bimodal age distribution at presentation; the first peak is seen in children and young adults and a second peak in patients over 50.
Pathologically there are two different types, adamantinomatous which is more often seen in the younger age group, and papillary type which is overall less common and generally presents in older patients. The adamantinomatous type demonstrates strands of epithelium defining adjacent loose hypocellular areas. It may also demonstrate regions of keratinization and calcification. The papillary type is described as a papillary organization of squamous epithelium without cyst formation or calcification.
The clinical presentation depends on size and location of the tumor. They may cause vision changes, headaches, hormonal imbalances or increased intracranial pressure.
Diagnosis can be suspected based on imaging findings but is confirmed by tissue analysis.
Craniopharyngiomas are generally suprasellar masses which may have intrasellar extension. Classic imaging findings include calcification, cyst formation, and solid enhancing components. Both CT and MRI are useful for characterization. CT is best for evaluation of the calcifications. On MRI, it is generally T1 isointense but there may be areas of increased T1 signal due to proteinaceous cyst contents. High T2 signal can be seen in the cystic components as well. There are generally solid enhancing components. The papillary type on the other hand tends to be more homogeneous in appearance without calcifications or cysts. It is generally T1 isointense and demonstrates enhancement.
Treatment options for craniopharyngiomas include surgery and radiation.
|
MRI and CT scan |
|
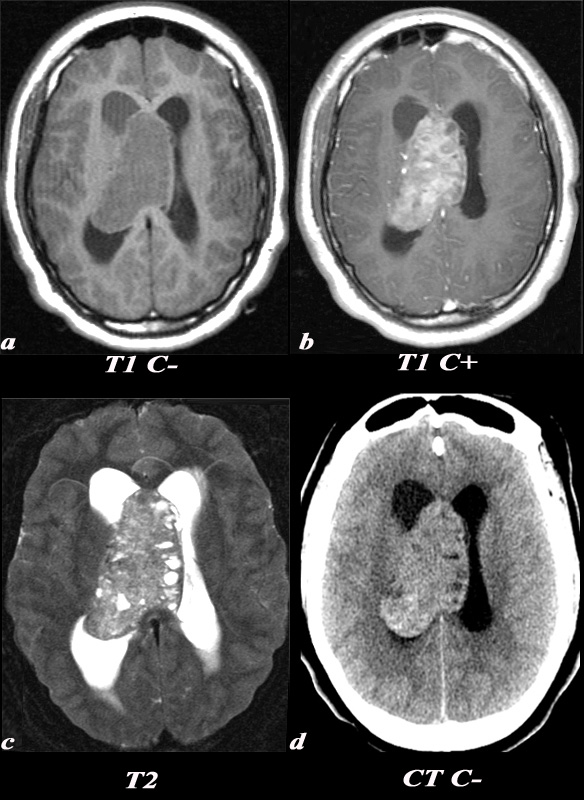
A 21 year old female was found to have papilledema on physical exam noted by her optometrist. MRI: T1 pre (T1 C- a) and post (T1 C+ b): Post contrast images demonstrate the heterogeneous enhancing nature of this mass. These images demonstrate centered in the right lateral ventricle with involvement of the septum pellucidum and partial extension into the left lateral ventricle. T2: T2 weighted images demonstrate internal areas of high signal consistent with cystic components. Also note the high T2 signal adjacent to the enlarged lateral ventricles which is a finding consistent with hydrocephalus, classically called transependymal flow of CSF. This unenhanced CT scan demonstrates also demonstrates the mass in the right lateral ventricle with similar features of heterogeneity and involvement of the septum pellucidum and partial extension into the left lateral ventricle. Notice the internal low density or cystic components and the higher density calcifications seen posteriorly. The lateral ventricles are enlarged consistent with resultant hydrocephalus. These findings are consistent with a diagnosis of central neurocytoma. Image Courtesy Elisa Flower MD and Asim Mian MD97634c01.8s |

H&E This medium power polymicrograph of tissue from a craniopharyngioma demonstrates findings typical of an adenomatous craniopharyngioma. The blue cells in the middle of the specimen are characteristic of squamous epithelium. If keratin staining were performed, it would be positive. The amorphous pink material at the lower right aspect of this image is consistent with necrobiosis or “wet keratin” from slowly degrading keratin. The purple focus at the left aspect of the specimen represents calcification, also characteristic of craniopharyngiomas.
H&E Craniopharyngioma |
|
The high power polymicrograph demonstrates several linear white areas consistent with cholesterol clefts (which have dissolved during preparation of the slide) which are also seen in craniopharyngiomas. C Image Courtesy of Cheryl Spencer, M.A. and Ivana Delalle, MD, PhD Department of Pathology Boston University School of Medicine 98490 98491b (S09-6977) |

References
Eldevik OP, Blaivas M, Gabrielsen TO, Hald JK, Chandler WF. Craniopharyngioma: radiologic and histologic findings and recurrence. AJNR Am J Neuroradiol 1996;17:1427-1439