
Hemangioblastoma
The Common Vein Copyright 2010
Definition
A hemangioblastoma is characterized as a benign, highly vascular tumor composed of abnormal vasculature with intervening stroma. They may be solid or solid with cystic components. They are most commonly found in the cerebellum but can also be seen in the spinal cord, medulla and cerebrum.
Pathologically, hemangioblastomas are made up of tightly packed blood vessels with intervening connective tissue. The vessel endothelial cells and stromal cells within the connective tissue generally demonstrate benign features without mitotic figures. There is usually no necrosis or hemorrhage. The “cyst” often associated with hemangioblastomas is not a true cyst in that there are no cells lining the wall, rather it is compressed brain parenchyma by the mass and fluid which may give this appearance.
There is an association between hemangioblastomas and the autosomal dominant disease von Hippel-Lindau. Approximately (40%) of patients with VHL develop a hemangioblastoma while (4040%%) of hemangioblastomas are associated with VHL.
Patients present clinically with a progressive, long term history of minor symptoms such as headache, disequilibrium, nausea and vomiting or dizziness. Many patients are found to have increased intracranial pressure secondary to obstructive hydrocephalus from the mass. Interestingly, hemangioblastomas may secrete erythropoietin and result in polycythemia.
Imaging of these tumors can be done by CT or MRI, which is more sensitive. Hemangioblastomas may have a solid or cyst with mural nodule appearance. At CT, the solid component is iso to hyperdense and demonstrates avid enhancement. The cystic component is hypodense. On MRI, the solid nodule demonstrates T1 iso to hypointensity and avidly enhances while the cystic component is T2 hyperintense. At angiography, hemangioblastomas may appear as a tangle of vessels or an area of dense tumor blush.
Treatment of hemagioblastomas consists of surgical resection for symptomatic cerebellar masses and laser therapy for retinal lesions.
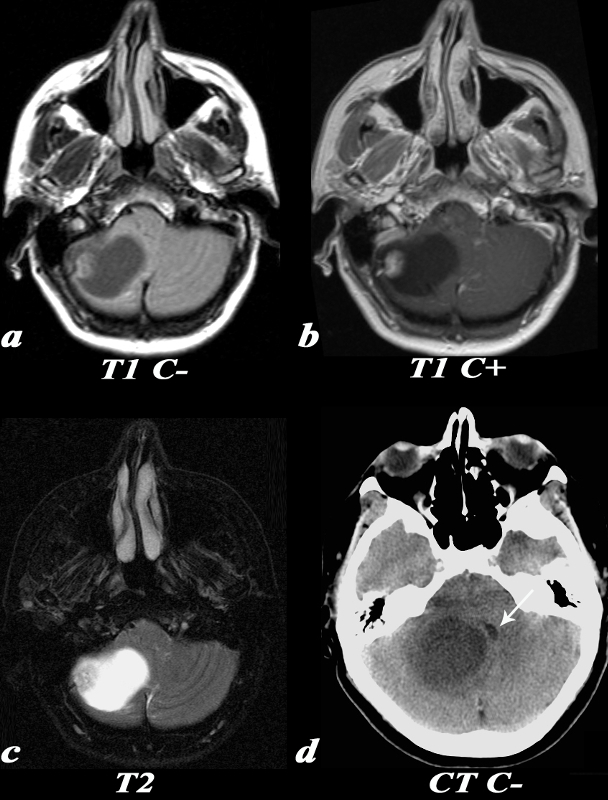
Hemangioblastoma – Nodule within a Cyst |
|
This 55 year old female complained of an occipital headache for one month with increased difficulty ambulating. MRI: T1 weighted images without contrast (a) demonstrate a T1 isointense nodule at the periphery of the lesion. Post contrast T1 weighted images (identified by high signal in the venous sinuses and high signal in the nasal mucosa due to normal enhancement) demonstrate enhancement of the nodular component of this tumor. The T2 weighted image demonstrates a predominantly T2 hyperintense cystic lesion with a nodular T2 isointense component seen laterally. CT: Noncontrast CT image demonstrates a large low density lesion in the right cerebellum. This lesion causes significant mass effect on the fourth ventricle which is displaced towards the left (white arrow). This mass effect caused obstruction of the CSF pathway resulting in obstructive hydrocephalus and subsequent symptoms. Image Courtesy Elisa Flower MD and Asim Mian MD 97652c.81 |
|
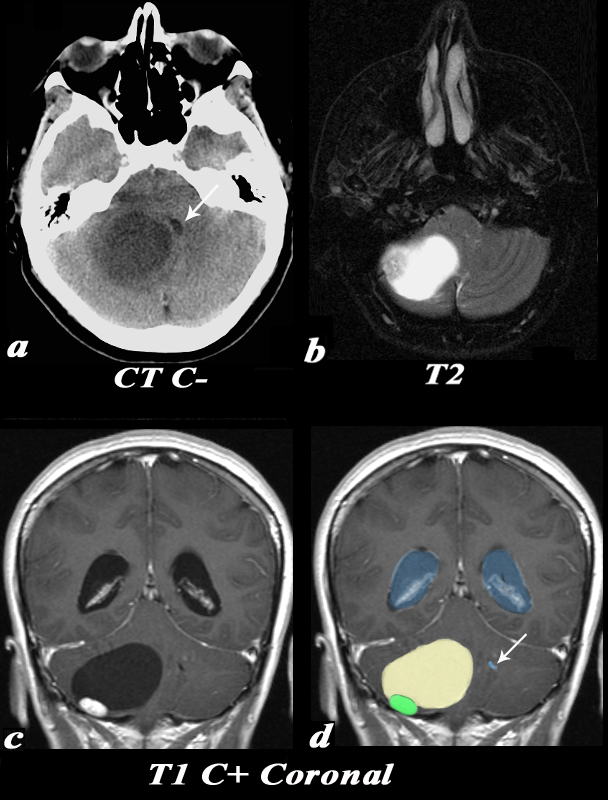
Hemangioblastom Causing Obstruction of the Fourt ventricle |
|
This 55 year old female complained of an occipital headache for one month with increased difficulty ambulating. CT: Noncontrast CT image (a) demonstrates a large low density lesion in the right cerebellum. This lesion causes significant mass effect on the fourth ventricle which is displaced towards the left (white arrow). This mass effect caused obstruction of the CSF pathway resulting in obstructive hydrocephalus and subsequent symptoms. MRI: The T2 weighted image (b) demonstrates a predominantly T2 hyperintense cystic lesion with a nodular T2 isointense component seen laterally. Post contrast T1 weighted coronal images (identified by high signal in the venous sinuses demonstrate the classic cyst (light yellow in d) with mural nodule (green in d) appearance of a hemangioblastoma. Note the enlarged lateral ventricles (blue) and the displaced and compressed 4th ventricle (white arrow d). Image Courtesy Elisa Flower MD and Asim Mian MD 97652c01.81 |

The lower power polymicrograph demonstrates a high vascular tumor with pleomorphic cells. H&E Low Power
On the high power polymicrograph, these cells are again, pleomorphic but benign in appearance. They have a bubbly appearing cytoplasm because they are lipidized. H&E High Power
Neuro Specific Enolase Immunohistochemical staining for neuron-specific enolase which is nonspecific for neurons is positive
Hemangioblastoma S-100 Immunohistochemical staining for neuron-specific enolase which is nonspecific for neurons is positive, as are some cells with S-100, which is also nonspecific for glial tumors.
|
|
Image Courtesy of Cheryl Spencer, M.A. and Ivana Delalle, MD, PhD Department of Pathology Boston University School of Medicine 98502/03/04/05 (S08-1356) |



—
References
Robbins
Ho, VB et al. Radiologic-Pathologic Correlation: Hemangioblastoma, AJNR 13:1343-1352. Sp/Oct 1992